
They span three continents, but a trio of researchers who’ve never met share a singular focus made vital by the still-raging pandemic: deciphering the causes of Long Covid and figuring out how to treat it.
Almost 2 years ago in Italy, pediatric infectious disease doctor Danilo Buonsenso, who works at Gemelli University Hospital, started to see children who, months after mild infections with SARS-CoV-2, were still short of breath and had crushing fatigue and other symptoms. He now suspects that, in some of them, the cells and tissues that control blood flow are damaged and the blood’s tendency to clot is amplified. Minute blood clots, leftover from the viral assault or fueled by its aftermath, might be gumming up the body’s circulation, to disastrous effect from the brain to joints. “In some patients we have specific areas where no blood flow comes in” or the flow is reduced, Buonsenso says. Is that driving their lingering symptoms? “I can’t say this is the truth, of course. But this makes sense.”
Meanwhile, in the United States, microbiologist Amy Proal can’t stop thinking about a second leading Long Covid theory: that the coronavirus keeps hurting people by stubbornly enduring in the body, even after acute infection passes. Studies have shown “the virus is capable of persistence in a wide range of body sites,” especially nerves and other tissues, says Proal, who works at the PolyBio Research Foundation, a nonprofit in Washington state. She recently caught COVID-19 for the third time.
Down under in Australia, immunologist Chansavath Phetsouphanh of the University of New South Wales, Sydney, is chasing a third lead, motivated by what the blood of Long Covid patients has divulged: an immune system gone haywire even 8 months after they’d first tested positive. He had assumed that immune cells galvanized to fight off infection would have calmed down over that time span. So, “It was a surprise that these cells did not recover,” says Phetsouphanh, who is working to set up an international Long Covid collaboration.
For each of these researchers—and many others exploring the causes of Long Covid—untangling the complex syndrome, with a still-evolving definition, is a laborious, step-wise process. First, they must show that a possible contributor—such as minuscule clots, lingering virus, or immune abnormalities—crops up disproportionately in people with Long Covid. Then comes the hard part: proving that each of these traits, alone or in combination, explains why the coronavirus has rendered millions of people shadows of their former selves.
All agree that solo operators are unlikely. Lingering virus, for example, could attack the circulatory system, triggering blood clots or chronic inflammation. “I see this as a triangle,” Buonsenso says, with each trigger potentially explaining, or even amplifying, the others.
A final challenge is identifying treatments that ease or reverse these abnormalities and help patients feel better. In the United Kingdom, home to a widely praised effort to identify immediate COVID-19 treatments, researchers are launching a clinical trial that will be among the largest worldwide to test potential Long Covid therapies in a randomized, statistically robust manner. But more such studies are needed—and time is of the essence. In May, the U.S. Centers for Disease Control and Prevention reported that a review of the medical records of nearly 2 million people suggested at least one in five of those diagnosed with COVID-19 had developed conditions characteristic of Long Covid. Other studies have found roughly similar rates. Some recent research suggests the risk for vaccinated people is somewhat lower, but vaccination’s power to head off the syndrome remains uncertain.
For Proal and others, fitting the puzzle pieces together is of urgent concern. “I consider Long Covid to be a massive emergency,” she says.
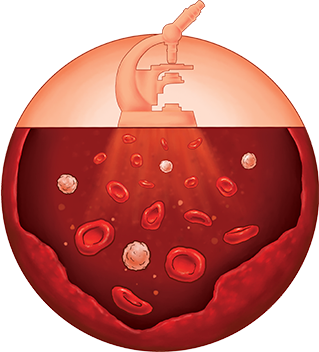
Tiny blood clots
A. MASTIN/SCIENCE
In Rome, Buonsenso is using a sophisticated medical imaging technique to better understand the role of blood clots. Called a SPECT-CT scan, it combines two different types of images: a single-photon emission computed tomography scan, which uses a radiotracer injected into a person’s veins to provide pictures of blood flow, and a standard CT scan for information about lung structure. By merging these, doctors can see which parts of the lungs aren’t getting normal blood flow.
So far, Buonsenso has scanned the lungs of 11 youngsters who have severe Long Covid, including irregular heartbeats and breathlessness during exercise. In six children, the lungs appeared normal. In the other five, the images were striking: Where there should have been bright oranges and yellows, signifying pulsing blood, one lung was nearly completely blue, indicating little flow. Buonsenso believes tiny blood clots or chronic damage to the lining of blood vessels may be impairing blood flow. He and his colleagues published their first evidence of such damage, in a 14-year-old girl, in July 2021 in The Lancet Child & Adolescent Health.
The knotty question is what to do next. Buonsenso’s patients don’t meet the current criteria for taking anticoagulant drugs that prevent blood clots or keep them from getting bigger, because no clots are visible on their scans. “You either say, ‘I’m sorry, but I can’t do anything outside of a study,’ or you are kind of a not-scared doctor with reciprocal trust with the patient and family, and together make a decision,” Buonsenso says.
With seriously ill children and their desperate parents in front of him, Buonsenso didn’t want to wait to launch a clinical trial. He and the families instead decided to do what they could. All five patients are now taking anticoagulants—which carry the risk of severe bleeding—under close monitoring.
He’s heartened by their progress. Several are back in school, playing sports, and spending time with friends. Two have been rescanned. A teenager who still suffers from symptoms showed little improvement. But in another, whose symptoms have largely resolved, the images looked nearly normal. The other three will be rescanned this summer.
Of course, he can’t be sure those who improved did so because of the treatment. That’s why he is hoping for resources to establish a Long Covid clinical trial that would include a placebo group.
Like other doctors, Buonsenso has been inspired by Long Covid patients who have lobbied hard for treatments and shared successes and failures on social media. Marta Esperti, a 34-year-old graduate student now living in Paris, is one of them. Struck by COVID-19 more than 2 years ago, she wasn’t hospitalized but months later struggled with fatigue, breathlessness when walking, persistent fever, joint pain, and other symptoms. Yet bloodwork and other medical tests, such as x-rays of her lungs, were largely normal. Esperti kept pushing for answers. Then, in the spring of 2021, “I received a call from the pulmonologist saying, ‘Listen, I want you to do another test.’”
Esperti was one of the first Long Covid patients in Europe to receive a lung SPECT-CT scan, and it looked just like the compromised lungs of the sick children Buonsenso scanned later. “My right lung is almost completely blue,” she says. She posted the images on Twitter, where they were shared by thousands of people.
Like Buonsenso, Esperti’s doctors believe damage to tiny blood vessels and minuscule clots are the culprit. The theory of persistent microclots gained further credence in the summer of 2021, when Resia Pretorius, a physiologist at Stellenbosch University in South Africa, and her colleagues reported in Cardiovascular Diabetology that such clots could linger in the blood of Long Covid patients. Her team found signs of excessive blood clotting in 11 people with Long Covid, but not in healthy people or another group with type 2 diabetes, whom they used for comparison.
One challenge facing clinicians keen to hunt for microclots in blood is that detecting them is a laborious process, although Pretorius is working to make it more accessible to doctors. SPECT-CT scans identify clots indirectly, based on blood flow abnormalities.
The work by Pretorius and others fits an emerging pattern in which the biology of acute and chronic COVID-19 appears to overlap. Early in the pandemic, doctors recognized blood clots as a signature of early, severe illness: Many hospitalized patients had clots in their lungs, brain, and elsewhere. Even people with milder disease were at heightened risk of heart attacks and strokes in the weeks following infection.
“The two diseases”—acute COVID-19 and Long Covid—“aren’t very different,” posits David Lee, an emergency medicine doctor at New York University Grossman School of Medicine. He suspects microclots explain many chronic symptoms. At least 70% of Long Covid patients have respiratory problems, he estimates, and at least 30% suffer from dysautonomia, in which abnormalities in the autonomic nervous system disrupt heart rate, breathing, and digestive function. Many suffer from fatigue and what’s often called “brain fog.” Tiny clots in the brain could explain cognitive troubles, Lee notes; or clots may kill small fiber nerve cells and drive dysautonomia.
But solid evidence that microclots cause Long Covid symptoms is still lacking. To learn more, Lee launched a study of 20 Long Covid patients with respiratory symptoms and 20 healthy volunteers who had COVID-19 and recovered. The participants will undergo SPECT-CT scans to see whether any of them have disrupted lungs. If abnormalities on the scans are unique to some with Long Covid, that could be a step toward identifying subsets of patients.
“I oscillate in my excitement” for different Long Covid theories, says David Putrino, a neurophysiologist and rehabilitation medicine specialist at the Icahn School of Medicine at Mount Sinai. He is studying several possible mechanisms for why symptoms can linger or even worsen after an infection. Right now, his enthusiasm for the microclot hypothesis is running high, thanks in part to a collaboration with Pretorius and others; that team has preliminary data to suggest the amount of microclots in blood correlates with the severity of some Long Covid symptoms, such as cognitive deficits.
Putrino is now running a small study of Long Covid patients with microclots in blood plasma, testing whether apheresis, which filters blood and reinfuses it, improves their symptoms. Any results, though, will be “very preliminary,” he cautions. Apheresis can “filter out lots of things in the blood” that also might fuel symptoms.
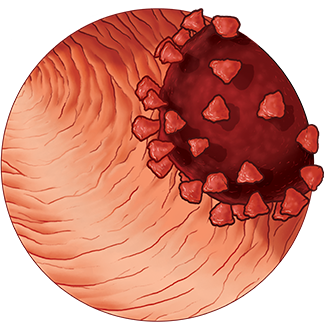
Persistent virus
A. MASTIN/SCIENCE
The idea that lingering virus might be a Long Covid culprit solidified for Proal in late 2021, thanks in part to an autopsy study that captured her attention. Researchers from the U.S. National Institutes of Health described in a preprint their analysis of tissues from 44 people who had been infected. Most had died from COVID-19 but five had mild or even asymptomatic infection and had succumbed to something else. All 44 still harbored viral RNA in their body, including in the brain, muscle, gut, and lungs. Many organs also had evidence of replicating virus.
The study established that replicating copies of the virus could persist. But it didn’t focus on people with Long Covid, making it difficult to establish a link.
Other studies are now trying to do that by comparing those with Long Covid and other cohorts, including people who have recovered from COVID-19. In one, gastroenterologist Herbert Tilg at the Medical University of Innsbruck set out to look for molecular traces of virus in the gut, a favorite hunting ground for researchers studying SARS-CoV-2. That’s because the gut is far easier for doctors to access than many other organs, such as the lungs or the brain, and is thought likelier to harbor virus than blood, which tends to clear a pathogen more quickly.
Tilg recruited 46 people who’d had COVID-19 months earlier, 21 of whom had at least one symptom of Long Covid. All the volunteers had inflammatory bowel disease and were scheduled for routine endoscopies. (Most were in remission.) Tilg used that procedure to gather extra tissue samples and probe for signs of the coronavirus. The bottom line: All of those with Long Covid symptoms harbored viral RNA or, in some cases, viral proteins. Among those who’d recovered from acute COVID-19, 11 had traces of virus, too, whereas another 14 had no virus that Tilg could find. He and colleagues published their study in May in Gastroenterology.
“Our paper is a clinical observation,” he stresses, and doesn’t prove that lingering virus is harming people. That said, Tilg was surprised by the presence of persistent virus in people with Long Covid symptoms, and its absence in many previously infected people who felt fine.
Now, researchers like Tilg want to understand how the small amounts of virus that linger in tissue reserves such as the gut behave. Tilg and Saurabh Mehandru, a gastroenterologist and immunologist at Mount Sinai who was among the first to find signs of persistent virus in COVID-19 survivors, haven’t been able to culture the virus from gut tissue in the lab—which would confirm that the virus is replicating. But such culturing can be tough, even in acute cases of COVID-19.
A key question is whether lingering virus is driving illness in Long Covid patients. Proal and her colleagues are trying to definitively tie persistent virus to Long Covid symptoms—or determine that the theory doesn’t hold water. She is working with Mehandru and with Putrino, who has access to a cohort of more than 1000 Long Covid patients who could participate in new studies. The team is planning colonoscopies to look for virus in intestinal cells, and also wants to scrutinize the activity of immune cells that populate the region. Are these cells in a heightened state of alert, for example, suggesting the viral particles are setting them off? In some patients, Mehandru has noted immune responses in the gut, but says the work is preliminary.
Ideally, this deep dive into the gut’s biology would be paired with a clinical trial examining whether antiviral drugs can beat back Long Covid symptoms. Participants could be studied before and after a course of antivirals, to see whether they clear any signs of virus in their gut and whether that matches up with changes in symptoms. “That’s the trial I’d love to see happen,” Putrino says.
So far it hasn’t, to the frustration of many in the Long Covid research and advocacy communities. “The patients are really, really desperate,” says Francisco Tejerina, an HIV researcher at Gregorio Marañón Hospital in Madrid, who has detected viral RNA in the stool, urine, and blood plasma of people with Long Covid. He worries about people experimenting on their own with therapies, including antivirals, that may be useless, or worse, dangerous. “They want something now,” he says. “I understand that.”
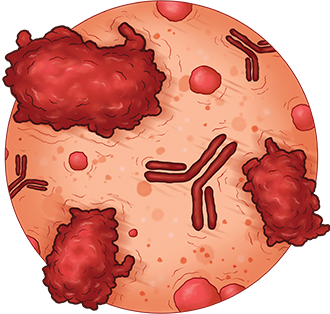
Haywire immune system
A. MASTIN/SCIENCE
As the pursuit of blood clots and viral fragments intensifies, a third track is both intersecting with those themes and making inroads on its own: the immune system, which some researchers believe could help bind together disparate observations. One idea, Phetsouphanh says, is that in some COVID-19 patients an immune system revved up and destabilized by the coronavirus attack may be unable to reset itself to idle.
To test that, he and colleagues gathered blood from 31 Long Covid patients, who all had fatigue or other characteristic symptoms at least 3 months after infection, and analyzed dozens of immune markers. “We were uncertain what we would find,” Phetsouphanh says. The result was striking. Essentially, Long Covid patients had an immune system in constant high alert, the team reported in January in Nature Immunology.
White blood cells that typically recruit other cells to sites of infection were highly activated, which may explain why the patients’ levels of interferons, proteins the body makes to fight invaders, were sky high 8 months after infection. The participants also had a dearth of inactivated T cells and B cells, a population of cells that normally putters about awaiting instruction to counter pathogens. Collectively this signaled chronic inflammation, which can cause a host of health problems.
Phetsouphanh and his colleagues also found these immune signatures were unique to their Long Covid cohort: They didn’t appear in people who’d had the virus but recovered, or in those who’d been infected with different coronaviruses.
Other groups are also finding myriad immune system abnormalities long after a SARS-CoV-2 infection. In January, immunologist Akiko Iwasaki at the Yale School of Medicine, neuroscientist Michelle Monje at Stanford Medicine, and their colleagues reported in a preprint that mice given the coronavirus in their nose to mimic a mild infection developed inflammation in the brain, as well as loss of myelin, which insulates nerves and helps them transmit signals. In the mice, inflammation struck the brain even though the researchers couldn’t find virus there. Furthermore, when the group compared blood samples from 48 people with Long Covid who had cognitive impairments and 15 Long Covid patients who did not, they found higher levels of inflammatory markers in the first group, suggesting chronic inflammation may be driving these neurological symptoms.
Such work highlights “how little we know about immune function,” says Putrino, who is collaborating with Iwasaki. Work like hers is “opening up this world” of immune markers that aren’t part of standard blood tests but may be critical to understanding the syndrome.
Increasingly, researchers want to fine-tune how they classify people with Long Covid, differentiating subsets based on symptoms, biology, or both. In a way, “the biggest obstacle that we are facing is we gave it one name, we gave it the name of Long Covid, which implies that it is one disease,” says Chahinda Ghossein, a physician and heart disease researcher at Maastricht University and co-leader of a 15,000-patient Long Covid study in the Netherlands. “All the studies being performed show us that it is not.”
One of the first large efforts to define subgroups, in part by testing potential treatments, will begin to enroll patients this month in the United Kingdom. Called STIMULATE-ICP (Symptoms, Trajectory, Inequalities and Management: Understanding Long-COVID to Address and Transform Existing Integrated Care Pathways), it will recruit 4500 Long Covid patients. Each will be randomly assigned one of three potential therapies: an anticlotting drug called rivaroxaban, an anti-inflammatory called colchicine, or a pair of antihistamines, famotidine and loratadine. (Antihistamines can quell a type of inflammation called mast-cell activation.) The project will include imaging as well as the collection of blood and tissue samples for a biobank. Organizers also have the option of adding up to three additional treatments.
Amitava Banerjee, a cardiologist at University College London, leads the study, and his colleague Emma Wall at UCL and the Francis Crick Institute is overseeing the treatment element. Both say it’s crucial to test Long Covid therapies in trials before prescribing them en masse to patients.
“If you follow social media, you might think we’ve cracked it,” Banerjee says, referring to anecdotal reports of vastly improved Long Covid symptoms, after, say, taking anticoagulants or antiviral drugs. Those narratives can offer important clues, he says, stressing that working with and listening to patients is invaluable. (Every component of STIMULATE-ICP includes a patient advocate.) But, “We’ve got to be really humble” about what we know, Banerjee adds.
After months of delays, the trial is “close to the start line,” he says, but “we should have been there months ago.” Trials for drugs to treat acute COVID-19 were fast-tracked, while “Long Covid is joining the queue with everything else” in medicine, Banerjee laments.
Esperti’s story underscores the work to be done. She’s been taking anticoagulant drugs for more than a year, and can now work, swim, drive, and cook—all previously impossible tasks. But she still can’t run or carry heavy objects, and she suffers from sporadic fatigue. She was hit by a second bout of COVID-19 in December 2021 that left her severely debilitated, but she improved after a fourth dose of vaccine in late March.
Mysteries remain. A repeat SPECT-CT scan 3 months after she started taking the drugs showed no change in her lungs, though her lung function has improved. “I thought all I have to do is take anticoagulants” and recovery would be quick, she says. Esperti suspects that, like peeling the layers of an onion, she’s unraveled one trigger for her symptoms only to come upon another she can’t yet decode. It’s another chapter in the annals of Long Covid—a narrative researchers are doggedly trying to change.
Leave a Reply