
News Release 29-Jul-2024
Peer-Reviewed Publication
Xia & He Publishing Inc.
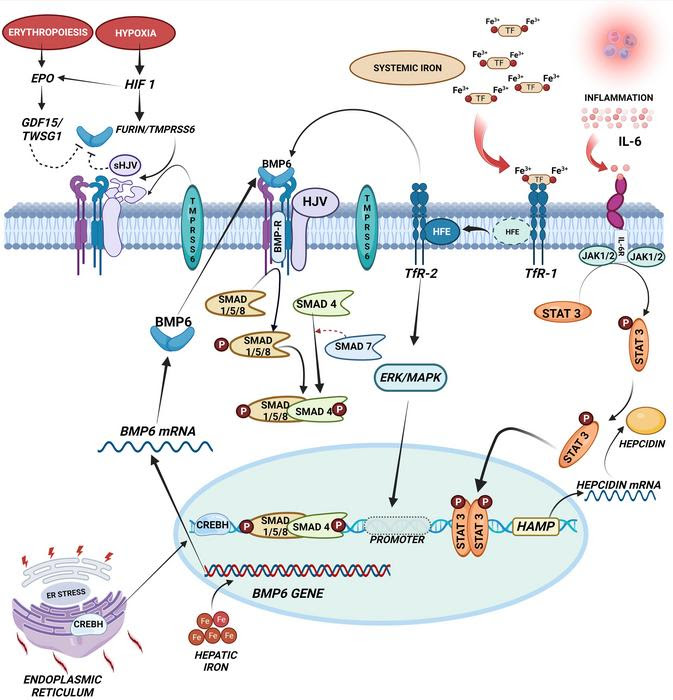
image:
Saturation of TfR1 leads to the dissociation of Hfe and the binding of the alter to the TfR2, which in turn influences the binding of BMP6 to its receptors on the membrane. Increased liver iron concentration induces the expression of the BMP6 gene, forming BMP6 proteins, which bind to the BMP receptors (ALK2). When bound to BMP6, the receptors recruit SMAD proteins and phosphorylation of SMAD1/5/8-SMAD4 complex mobilizes to the nucleus, activating the expression of hepcidin. Inflammatory signals via IL-6 through the JAK-STAT cascade induce the expression of the Hepcidin gene (HAMP). Higher EPO and HIF lead to the secretion of ERFE from erythroid precursor cells, which attenuates the BMP6 signaling cascade via GDF15/TWSG1. In the absence of BMP6, TMPRSS6 binds to ALK2, inhibiting the hepcidin signaling cascade. BMP6, bone morphogenic protein 6; EPO, erythropoietin; ERFE, erythroferrone; Erk, extracellular signal-regulated kinase; GDF15, growth differentiation factor15, HAMP, hepcidin antimicrobial peptide; Hfe, hemochromatosis gene; HIF, hypoxia-induced factor; IL-6, interleukin 6; JAK-STAT, Janus kinase/signal transducer and activator of transcription; MAPK, mitogen-activated protein kinase; mRNA, messenger RNA; sHJV, soluble hemojuvelin ; SMAD, mothers against decapentaplegic; TfR1/2, Transferrin receptor; TMPRSS6, transmembrane serine protease 6; TWSG1, twisted gastrulation factor1.
Credit: Akila Prashant
β-Thalassemia is a genetic disorder characterized by reduced or absent synthesis of the beta chains of hemoglobin, leading to ineffective erythropoiesis and severe anemia. Patients with transfusion-dependent β-thalassemia (TDT) require regular blood transfusions to maintain adequate hemoglobin levels. Non-transfusion-dependent thalassemia (NTDT) patients manage their anemia without regular transfusions but still experience significant health complications. Iron overload is a common and severe complication in both TDT and NTDT patients due to increased intestinal iron absorption and regular transfusions. The excess iron accumulates in vital organs, including the liver, heart, and endocrine glands, causing significant morbidity and mortality. This review explores the mechanisms of iron overload in β-thalassemia, current diagnostic and monitoring techniques, and advances in management strategies.
Mechanisms of Iron Overload
In β-thalassemia, iron overload occurs through two primary mechanisms: transfusional iron overload in TDT patients and increased gastrointestinal iron absorption in NTDT patients due to ineffective erythropoiesis and low hepcidin levels. Hepcidin, a liver-derived hormone, regulates iron homeostasis by inhibiting intestinal iron absorption and iron release from macrophages. In β-thalassemia, hepcidin levels are inappropriately low, leading to excessive iron absorption. This dysregulation results in systemic iron overload. The iron overload leads to the production of reactive oxygen species (ROS) through iron-mediated Fenton reactions, contributing to oxidative stress and tissue damage. Chronic iron overload is particularly detrimental to the liver, heart, and endocrine organs, leading to fibrosis, cardiomyopathy, and endocrine dysfunctions, respectively.
Diagnosis and Monitoring
Diagnosing iron overload involves several parameters, with serum ferritin levels being a primary indicator. Elevated serum ferritin levels, typically above 300 ng/ml in males and 150–200 ng/ml in females, signal excess iron accumulation. However, inflammation, infection, and liver disorders can affect ferritin levels, necessitating the use of additional markers such as total iron binding capacity, serum transferrin saturation, and non-transferrin-bound iron (NTBI). Magnetic resonance imaging (MRI) has replaced liver biopsy for non-invasive quantification of hepatic iron overload and can also assess iron accumulation in the heart and other organs. T2* MRI is particularly useful for evaluating cardiac iron overload and guiding chelation therapy adjustments. Liver iron concentration (LIC) measurement through R2 and R2* MRI techniques provides a reliable assessment of hepatic iron burden.
Management Strategies
The primary treatment for iron overload is chelation therapy, which involves the use of agents such as deferoxamine, deferiprone, and deferasirox to bind excess iron and facilitate its excretion. Chelation therapy’s efficacy depends on patient adherence, which can be affected by side effects and cost. Deferoxamine, administered via subcutaneous or intravenous infusion, is effective but burdensome for patients. Oral chelators such as deferiprone and deferasirox offer more convenience, improving compliance. Emerging therapies aim to enhance chelation efficiency and reduce side effects. These include the development of new chelators, combination therapies, and the use of plant extract derivatives with antioxidant properties. Combination therapy, using deferiprone and deferoxamine, has shown synergistic effects, improving iron removal and reducing toxicity.
Future Perspectives
Research is focused on understanding the molecular mechanisms underlying iron overload and developing targeted therapies. Advances in genetic and molecular screening have improved our understanding of genotype-phenotype correlations in thalassemia. Techniques such as next-generation sequencing (NGS) enable the identification of mutations in genes regulating iron metabolism. Innovations in gene editing, such as CRISPR-Cas9, hold promise for correcting genetic defects responsible for iron overload. Additionally, nanoparticle-based delivery systems offer potential for targeted therapy, reducing systemic toxicity and improving therapeutic outcomes. Hepcidin mimetics and modulators are also being investigated to restore hepcidin levels and regulate iron absorption effectively.
Conclusions
Iron overload remains a significant challenge in the management of β-thalassemia. Early diagnosis and regular monitoring are crucial for preventing organ damage. While chelation therapy is the cornerstone of treatment, its limitations necessitate the exploration of novel therapeutic strategies. Advances in molecular genetics and targeted therapies offer hope for more effective management of iron overload in β-thalassemia patients. Personalized treatment approaches, informed by genetic and molecular profiling, are essential for optimizing patient outcomes. Continued research and clinical trials are vital to developing safer, more effective treatments and improving the quality of life for β-thalassemia patients worldwide.
Full text
https://www.xiahepublishing.com/1555-3884/GE-2023-00128
The study was recently published in the Gene Expression.
Gene Expression (GE) is an open-access journal. It was launched in 1991 by Chicago Medical School Press, and transferred to Cognizant Communication Corporation in 1994. From August 2022, GE is published by Xia & He Publishing Inc.
GE publishes peer-reviewed and high-quality original articles, reviews, editorials, commentaries, and opinions on its primary research topics including cell biology, molecular biology, genes, and genetics, especially on the cellular and molecular mechanisms of human diseases.
GE has been indexed in Medline (1991-2021), Scopus, Biological Abstracts, Biosis Previews, ProQuest, etc.
Follow us on X: @xiahepublishing
Follow us on LinkedIn: Xia & He Publishing Inc.
Journal
Gene Expression
DOI
10.14218/GE.2023.00128
Article Title
Exploring the Impact of Iron Overload on Mitochondrial DNA in β-Thalassemia: A Comprehensive Review
Article Publication Date
15-Apr-2024
Leave a Reply