
September 11, 2024
by Jennifer Michalowski, Massachusetts Institute of Technology
Credit: Current Biology (2024). DOI: 10.1016/j.cub.2024.08.004
Placebos are inert treatments, generally not expected to impact biological pathways or improve a person’s physical health. But time and again, some patients report that they feel better after taking a placebo. Increasingly, doctors and scientists are recognizing that rather than dismissing placebos as mere trickery, they may be able to help patients by harnessing their power.
To maximize the impact of the placebo effect and design reliable therapeutic strategies, researchers need a better understanding of how it works. Now, with a new animal model developed by scientists at the McGovern Institute at MIT, they will be able to investigate the neural circuits that underlie placebos’ ability to elicit pain relief.
“The brain and body interaction has a lot of potential, in a way that we don’t fully understand,” says Fan Wang, an MIT professor of brain and cognitive sciences and investigator at the McGovern Institute. “I really think there needs to be more of a push to understand the placebo effect, in pain and probably in many other conditions. Now we have a strong model to probe the circuit mechanism.”
Context-dependent placebo effect
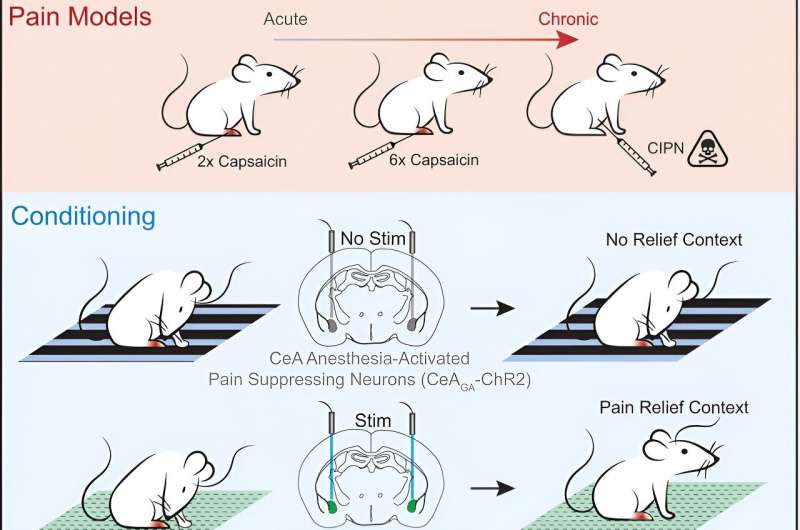
In the Sept. 5, 2024, issue of the journal Current Biology, Wang and her team report that they have elicited strong placebo pain relief in mice by activating pain-suppressing neurons in the brain while the mice are in a specific environment, thereby teaching the animals that they feel better when they are in that context.
Following their training, placing the mice in that environment alone is enough to suppress pain. The team’s experiments show that this context-dependent placebo effect relieves both acute and chronic pain.
Context is critical for the placebo effect. While a pill can help a patient feel better when they expect it to, even if it is made only of sugar or starch, it seems to be not just the pill that sets up those expectations, but the entire scenario in which the pill is taken. For example, being in a hospital and interacting with doctors can contribute to a patient’s perception of care, and these social and environmental factors can make a placebo effect more probable.
MIT postdocs Bin Chen and Nitsan Goldstein used visual and textural cues to define a specific place. Then they activated pain-suppressing neurons in the brain while the animals were in this “pain-relief box.”
Those pain-suppressing neurons, which Wang’s lab discovered a few years ago, are located in an emotion-processing center of the brain called the central amygdala. By expressing light-sensitive channels in these neurons, the researchers were able to suppress pain with light in the pain-relief box and leave the neurons inactive when mice were in a control box.
Animals learned to prefer the pain-relief box to other environments. And when the researchers tested their response to potentially painful stimuli after they had made that association, they found the mice were less sensitive while they were there.
“Just by being in the context that they had associated with pain suppression, we saw that reduced pain—even though we weren’t actually activating those [pain-suppressing] neurons,” Goldstein explains.
Acute and chronic pain relief
Some scientists have been able to elicit placebo pain relief in rodents by treating the animals with morphine, linking environmental cues to the pain suppression caused by the drugs similar to the way Wang’s team did by directly activating pain-suppressing neurons.
This drug-based approach works best for setting up expectations of relief for acute pain; its placebo effect is short-lived and mostly ineffective against chronic pain. So Wang, Chen, and Goldstein were particularly pleased to find that their engineered placebo effect was effective for relieving both acute and chronic pain.
In their experiments, animals experiencing a chemotherapy-induced hypersensitivity to touch exhibited a preference for the pain relief box as much as animals who were exposed to a chemical that induces acute pain, days after their initial conditioning. Once there, their chemotherapy-induced pain sensitivity was eliminated; they exhibited no more sensitivity to painful stimuli than they had prior to receiving chemotherapy.
One of the biggest surprises came when the researchers turned their attention back to the pain-suppressing neurons in the central amygdala that they had used to trigger pain relief. They suspected that those neurons might be reactivated when mice returned to the pain-relief box.
Instead, they found that after the initial conditioning period, those neurons remained quiet. “These neurons are not reactivated, yet the mice appear to be no longer in pain,” Wang says. “So it suggests this memory of feeling well is transferred somewhere else.”
Goldstein adds that there must be a pain-suppressing neural circuit somewhere that is activated by pain-relief-associated contexts—and the team’s new placebo model sets researchers up to investigate those pathways.
A deeper understanding of that circuitry could enable clinicians to deploy the placebo effect—alone or in combination with active treatments—to better manage patients’ pain in the future.
More information: Bin Chen et al, Reverse-engineering placebo analgesia, Current Biology (2024). DOI: 10.1016/j.cub.2024.08.004
Journal information: Current Biology
Provided by Massachusetts Institute of Technology
Leave a Reply