
by St. George’s University of London
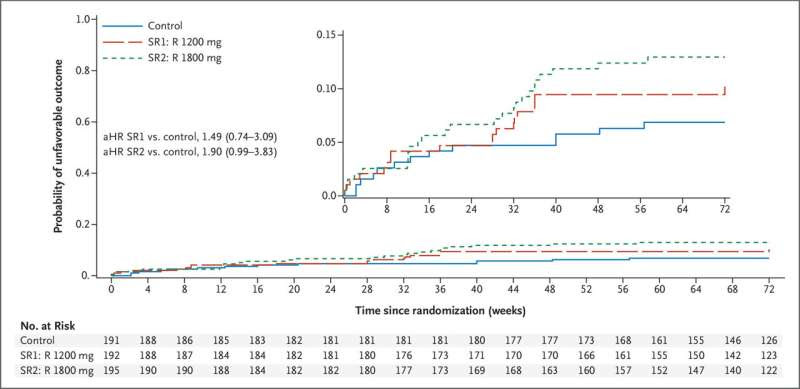
Kaplan–Meier Time to Unfavorable Outcome for the Primary mITT-M Population. The inset shows the same data on an enlarged y axis. aHR denotes adjusted hazard ratio; mITT-M, modified intention-to-treat microscopy positive; R, rifampicin; SR1, study regimen 1; and SR2, study regimen 2. Credit: NEJM Evidence (2023). DOI: 10.1056/EVIDoa2300054
A higher dose and shorter treatment time of a cornerstone tuberculosis (TB) drug has proven to be safe for patients, according to a clinical trial led by researchers at St George’s, University of London. Results have been published in NEJM Evidence.
The researchers found that a higher dose of the antibiotic rifampicin given for a shortened treatment time of just four months, compared to the standard six months, was safe with no increase in side effects or toxicities.
TB has the highest death rate of all infectious diseases—above and beyond COVID-19. There are an estimated 10 million new cases of TB every year, with 4.3 million thought to be undiagnosed.
Hopes for better adherence to treatment
Researchers anticipate that a shorter treatment period is fundamental in increasing the compliance rate of those taking anti-TB drugs, to ultimately lead to more cures, reduced transmission, lower chance of developing resistance and fewer deaths.
The WHO-recommended standard treatment for TB is currently a six-month regimen which includes the key antibiotic, rifampicin. This has proven to be highly effective at curing TB, but the number of patients adhering to their daily medication is sub-optimal due to the long time frame, leading to a recurrence in their disease. This presents a major challenge in treating TB.
Mission to eradicate TB
Professor Amina Jindani, Emeritus Professor of Tuberculosis Therapeutics at St George’s, University of London, who led the trial said, “In the absence of an effective vaccine, I believe that making TB treatment as accessible as possible and reducing its duration from the current six months are our best options for eradicating the disease across the world. Our research now presents a major milestone for TB treatment as it proves that a higher dose of widely available drugs over just four months is possible and safe.
“This is good news for people diagnosed with TB—it simplifies their treatment meaning they are more likely to complete the full course, giving them the best chance of being cured, while slashing the cost which is a huge barrier in developing countries.”
Rifampicin works by killing the Mycobacterium tuberculosis bacteria undergoing rapid metabolism and kills the persistent mycobacteria thought to be responsible for most relapses.
Adults with newly diagnosed pulmonary tuberculosis were recruited to the Rifashort trial between 2017–2020 in centers across Uganda, Guinea, Peru, Nepal, Botswana and Pakistan. People were excluded from the trial if they had previously undergone more than one week of treatment, were HIV-positive, had pre-existing liver disease or diabetes, or had drug resistance to rifampicin and/or isoniazid.
From six to four months
A total of 578 people were randomly assigned to receive either the standard daily six-month treatment of rifampicin at 600 mg (191 people), a higher dose over four-months of rifampicin at 1200 mg (192 people) or 1800 mg (195 people). Rifampicin was given along with standard doses of other first-line anti-TB drugs (isoniazid, ethambutol and pyrazinamide) for the first two months. Patients were followed-up monthly for the first 12 months after starting treatment and then at 15 and 18 months.
Sputum and blood samples were collected and analyzed to determine if treatment was killing the bacteria.
The number of participants who maintained a TB culture negative status (showing the treatment was killing the bacteria) by the end of the follow-up period with no adverse effects were 93%, 89.8% and 86.6% for the control, 4-month 1200 mg, and 4-month 1800 mg groups, respectively. Adverse events occurred in 4%, 4.5% and 4.4%, respectively.
Although the shorter treatment groups didn’t meet the level of desired outcomes when compared with the control group, the researchers emphasize the importance of the results in pushing TB care forward. They say the results provide evidence that a shorter regimen is possible but anticipate it would be most effective for people diagnosed in the earlier stages of the disease.
A tailored approach
Professor Thomas Harrison, Professor of Infectious Diseases and Medicine at St George’s, University of London said, “We now want to take a more tailored approach to the treatment of TB based on disease severity. We suspect that the four-month 1200mg dose will greatly benefit people living with an earlier form of TB, whereas those who have more extensive disease might respond best to a high, six-month dose.
“To explore this we hope to use a new GeneXpert tool at our treatment centers so they can immediately determine patients’ TB severity and put them onto the most effective treatment plan for them without delay.”
Professor Amina Jindani added, “Africa and poorer countries bear the brunt of the disease but there’s no room for complacency in the U.K., Europe or North America as large-scale migration and travel continue to pose a challenge to our ultimate goal of eradicating the disease. That’s why it’s vital we continue our research to find the most effective therapies which are accessible to countries worldwide.”
More information: Amina Jindani et al, Four-Month High-Dose Rifampicin Regimens for Pulmonary Tuberculosis, NEJM Evidence (2023). DOI: 10.1056/EVIDoa2300054
Journal information: NEJM Evidence
Provided by St. George’s University of London
Leave a Reply